The Post-Gleevec Era
Gleevec (imatinib) was the first tyrosine kinase inhibitor approved for the treatment of cancer and one of the first products to emerge from "rational drug design." It's invention changed chronic myeloid leukemia from an incurable death sentence to a manageable disease. Here's a look back on the tremendous value it's created over the last two decades.
It's hard to imagine that only twenty years ago, kinases were considered "undruggable". The biggest problem in many kinase programs today is finding novel inhibitors, since so many groups have successfully patented inhibitors of the highly-conserved ATP-binding domain. But pre-Gleevec, the worry was kinase inhibitors would be toxic because it would be impossible to target only one. Achieving low drug doses would also be difficult because of the high concentrations of intracellular ATP. Even if you could find the perfect drug, it was unclear if knocking out a single kinase would really affect a disease, given the complexity of the signalling networks kinases are embedded within. Finally, the only indications that would tolerate the expected small window for efficacy over toxicity were cancers - so unless you basically cured a cancer, there was unlikely to be a market for your drug. (Indeed, the vast majority of clinical kinase inhibitors are approved in cancer: (Hantschel, O. ACS Chem. Biol. 2015, 10, 234-245.) Don't get me wrong — these are valid concerns. Demonstrating selectivity, safety, potency, and efficacy with new kinase inhibitors is still hard. It's just that Gleevec's success was proof it could be done, and inspired teams targeting kinases and other challenging targets. Now that imatinib is finally going generic, it's a great time to reflect on the value it's created so far in its lifecycle, and remember why we should go after what's hard.


Each red circle on the dendrogram represents activity against a different kinase (larger circles = more potent). The natural product Staurosporine, originally reported to inhibit PKC, was later discovered to inhibit a vast array of kinases. No wonder the development of a more selective compound like imatinib seemed daunting. Image generated using TREEspot™ Software Tool and reprinted with permission from KINOMEscan®, a division of DiscoveRx Corporation, © DISCOVERX CORPORATION 2010.
Chronic Myeloid Leukemia - Before and After
Chronic myeloid leukemia (CML) was once a fatal disease, with a median survival of 3-5 years. As Dr. Kantarjian recounts in The Emperor of All Maladies, "Before the year 2000, when we saw patients with chronic myeloid leukemia, we told them that they had a very bad disease, that their course was fatal, their prognosis was poor with a median survival of maybe three to six years, frontline therapy was allogenic transplant... and there was no second line treatment..." (An unparalleled, inspirational, and authoritative masterpiece on cancer: (Mukherjee, Siddhartha. The Emperor of All Maladies: A Biography of Cancer. New York: Scribner, 2010. Print.)
"Today when I see a patient with CML, I tell them that ... they will usually live their functional life span provided they take an oral medicine, Gleevec, for the rest of their lives."
Today, the phrases "pre-Gleevec era" and "post-Gleevec era" are commonly used by oncologists when discussing treatment of CML. Less than two decades after imatinib's FDA approval, CML patients on imatinib are expected to have a near-normal life expectancy, with >80% of patients with CML are still alive 10 years after starting the oral treatment. Again quoting Dr. Kantarjian, "Today when I see a patient with CML, I tell them that the disease is an indolent leukemia with an excellent prognosis, that they will usually live their functional life span provided they take an oral medicine, Gleevec, for the rest of their lives."
Sailing Against the Winds
Chronic myeloid leukemia (CML) was once a rare disease, affecting only ~5000 new patients per year in the US. This made it difficult for major companies to justify risking hundreds of millions on clinical development, especially with unproven drugs for a new target class. Modern trials continue to show that when you try to fight cancer, you usually lose, and companies can't simply risk throwing away large sums which could be invested fighting diseases which affect many others. It certainly wasn't clear imatinib would work. Sure, preclinical data showed imatinib suppressed the growth of Bcr-Abl+ cell lines in a Petri dish over a few days, but even then it did not always lead to killing of 100% of Bcr-Abl+ tumor cells. Real leukemias, unlike the Petri dish models, might not totally depend on Bcr-Abl+ for survival, and could develop Bcr-Abl-independent methods of growth over a short period of time, rendering treatment inconsequential in the long run. Imatinib would have to suppress tumor growth for years to make a difference in a CML patient's life, and there's no model for that but a long and expensive clinical trial.
"However, if this compound proves too toxic in vivo, another possible use would be in vitro purging of Bcr-Abl-expressing cells for use in autologous bone marrow transplantation."
It definitely wasn't clear imatinib would be safe for one week, let alone for five years. A credible paper had demonstrated that suppression of c-Abl, the target of imatinib, was likely to lead to hematopoetic toxicities. (Caracciolo, D. et al. Science, 1989, 245, 1107-1110.) Even though the imatinib team demonstrated that in contrast to c-Abl anti-sense oligonucleotides, imatinib did not suppress hematopoetic colony formation in vitro and was safe in animals, they could not be completely confident imatinib would be safe in humans. In fact, the imatinib team even suggests a backup plan to simply use imatinib as a tool to treat cells ex vivo for autologous bone marrow transplant if it turned out to be poorly tolerated! Quoting their original paper, "However, if this compound proves too toxic in vivo, another possible use would be in vitro purging of Bcr-Abl-expressing cells for use in autologous bone marrow transplantation." (Druker, B. J. et al., Nature Medicine, 1996, 2, 561-566.)
A Different Kind of Emerging Market

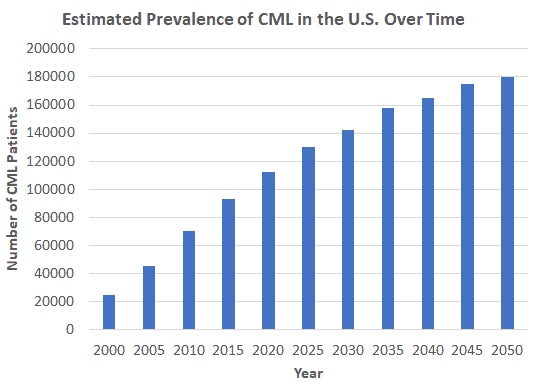
Estimated number of patients living with CML over time in the U.S. based on an incidence rate of 4,800-5,200 cases per year and a post-Gleevec era 10-year all-cause mortality rate of 2%.
An Unexpected Blockbuster
Imatinib and second-generation tyrosine kinase inhibitors like dasatinib and nilotinib have clearly made a tremendous impact in the lives of hundreds of thousands of patients and their families. But one question that nearly killed the program from the outset was, would a therapy for such a small subset new cancers per year (~5000) ever be able to return the cost of its development if it turned out to work? This continues to be a serious question for all new targeted therapy programs, but we at least know in retrospect that for tyrosine kinase inhibitors like Gleevec, the answer is a resounding yes. The graph below shows the net sales of Gleevec and 2nd-generation TKIs by year, compiled from Novartis and Bristol-Myers Squibb's annual reports. In its first two years on the market alone, Gleevec returned net sales of >$1 billion. Sales continued to grow year on year, reaching a peak of >$4.6 billion net sales by 2012. This speaks to the tremendous value created by an agent which has effectively cured a cancer. What other industry could claim a feat like this?

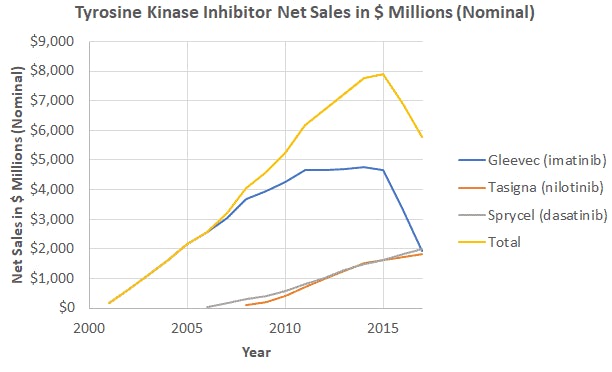
Net sales of imatinib and 2nd-generation tyrosine kinase inhibitors since imatinib's approval in 2001.
Gross sales of dasatinib are shown. Imatinib finally went off-patent in 2015, and Gleevec's net sales have slumped since. But in total, Gleevec returned a cumulative $51 billion in net sales (nominal), and saved countless lives and hospitalizations in the process. Second generation tyrosine kinase inhibitors like Sprycel (dasatinib) and Tasigna (nilotinib), which are active against imatinib-resistant CML, have generated an additional ~$20 billion in net sales. Note that while the patent protection for all of these drugs and hence the revenue streams from these drugs will be expiring, a functional cure for chronic myeloid leukemia exists forever. Talk about a return on investment! To put it in perspective, let's compare the cumulative lifetime sales of imatinib from 2001-2017 to some other big numbers. The lifetime net sales of this one product dwarfs the value of some "unicorn" biotech buyouts (Flexus, $1.25 billion, Stemcentryx, $10.2 billion), and could have paid for the acquisition of a large-cap company like Genentech ($46.7 billion). On the other hand, the sales over 17 years pales in comparison to only one year of iPhone net sales. Some final food for thought: Facebook today is worth more than 10x the total profits returned by imatinib.

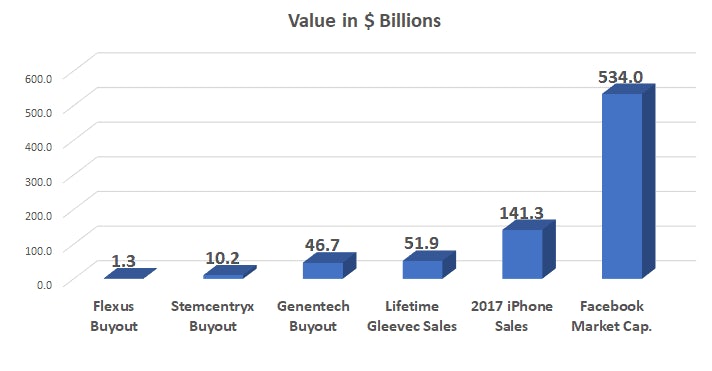
A comparison of Gleevec sales over its patented lifetime (2001-2017) to other high-value items. Note that one year of iPhone net sales dwarfs the net sales ever achieved by Gleevec. On the other hand, the net sales of Gleevec alone could have paid for nearly fifty unicorn biotech buyouts, or the outright purchase of Genentech in 2009.
Lessons for Drug Hunters
George Merck once said about the pharmaceutical business, "We try never to forget that medicine is for the people. It is not for the profits. The profits follow, and if we have remembered that, they have never failed to appear." The development of imatinib is a prime example supporting this ethos. Though its wild success has been difficult to replicate by other drugs in the years since its approval, it serves as a powerful reminder of why hard problems in drug discovery and development are worth the fight to take them down. What targets will be the "kinases" of the post-Gleevec world? Phosphatases? E3-Ligases? There are many challenges waiting for us, but thanks to those who came before, we can imagine what success might look like. Explore drughunter.com for more.